We are pleased to announce that we are now able to offer Telehealth or Virtual Osteopathic Consultations! Unfortunately, we are not currently accepting any in-person osteopathic consultations. We are following recommended guidelines and will notify our patients as soon as we are able to accept in-person appointments.
ABOUT VIRTUAL CARE
Access to healthcare services can my all the difference in the world – especially during these unprecedented times. The way of the world has changed, and we must adapt with it. With in-person services not currently available, we are still able to provide the highest quality of care through our telehealth or virtual care services at a distance.
Our telehealth services are easy to use, secure, safe and convenient.
HOW IT WORKS
Prior to your appointment, you will receive an email or text link to your appointment session. This will enable both audio and video connection between you and the clinician. Any documentation that you need to review and complete prior to your appointment will be sent to you ahead of time.
If at any time during the session, we believe that an in-person appointment is urgent, we will provide appropriate guidance and referrals.
WHAT TO EXPECT DURING YOUR TELEHEALTH OR VIRTUAL CONSULTATION
At the beginning of your telehealth consultation, the clinician will review your case, obtain consent to participate in the session via the secure platform.
Just like an in-person consultation, the clinician will listen to the patient’s chief complaint, concerns and current status.
The clinician will then perform an assessment. The patient may be asked to perform specific movements or orthopedic tests to help determine the osteopathic diagnosis.
Once the clinician is confident in the proper diagnosis, a treatment plan will be recommended. The treatment plan can include but is not limited to the following:
A thorough explanation of the condition/ injury.
What to expect and the prognosis.
A treatment plan which you can provide in the comfort of your home using the tools the patient has available such as electrotherapy, rest/activity, ice/heat, self therapy mobilizations, and therapeutic exercises.
Any questions the patient may have will be answered to the best of our ability.
Once the patient and the clinician have agreed upon the provided treatment plan, the clinician will recommend any necessary follow up appointments which will be scheduled accordingly.
After the consultation has completed, the clinician will email the documented treatment plan to the patient which will entail a full description of the condition being treated, the detailed treatment plan provided, a pdf download of the therapeutic exercises prescribed as well as a direct link to review the video of the therapeutic exercises prescribed.
EVER WONDERED IF YOU SHOULD USE HEAT OR ICE FOR YOUR PAIN OR INJURY? HERE IS YOUR GUIDE!
The most simplest and general way to put it is… if you have an acute injury use ice and if you have a chronic injury use heat. BUT, it can get more complex.
The following is a simple guide from the Cleveland Clinic to help you decide if ice or heat is right for your condition.
I will be writing an article this week on the R.I.C.E principle for acute injuries this week which will help you understand why the physician that coin the phrase in 1978 is taking a step back now in regards to that Rest and Ice aren’t necessarily the best treatments for acute injuries!
As the number of cases of COVID-19 in our region and Country increase, we have decided it is in our communities best interest to continue to seize operations until further notice by our colleges, associations, Health Canada and government officials.
If you need any advice or guidance for acute injuries or chronic pain management, please reach out to us. We will be able to guide you the best we can through email, phone, video if need be. Some clinics are charging patient’s for this service but we will be doing this at no cost at this time.
My personal number is 519-551-3463 (cell) and email is spencerjean_do@outlook.com. Reach out via text or email if you have any questions, comments or concerns!
Please follow our government officials advice in handling Covid-19. If everyone does their part, we will be able to get back to normal sooner! We miss all of our patient’s and delivering the highest standard of care to them.
It may surprise you to learn that 75% of Americans are Chronically Dehydrated. A survey of 3,003 Americans found that 75 percent likely had a net fluid loss, resulting in chronic dehydration [i].
Water is the most vital compound for any living organism. It constitutes up to 70% of the total body weight, depending on age, gender, and body composition. Water is the main component of all fluids in the body and involves almost in every functions of the body.
Body Composition:
Water
60%
Proteins
18%
Fats
15%
Minerals
4%
Carbohydrates
2%
Vitamins
1%
AVERAGE BODY COMPOSITION
WATER LOSS
An average person with little or no exercise loses about 2200 ml (2.2 L) of water daily. For the daily water loss, see the table below [ii].
DEHYDRATION EFFECTSON YOUR BODY [iii]
PHYSICAL PERFORMANCE
During challenging athletic events, it is not uncommon for athletes to lose 6–10% of body weight in sweat loss, thus leading to dehydration if fluids have not been replenished. However, decrements in physical performance in athletes have been observed under much lower levels of dehydration, as little as 2%.
Under relatively mild levels of dehydration, individuals engaging in rigorous physical activity will experience decrements in performance related to reduced endurance, increased fatigue, altered thermoregulatory capability, reduced motivation, and increased perceived effort.
COGNITIVE PERFORMANCE
Water, or its lack (dehydration), can influence cognition. Mild levels of dehydration can produce disruptions in mood and cognitive functioning.
As with physical functioning, mild to moderate levels of dehydration can impair performance on tasks such as short-term memory, perceptual discrimination, arithmetic ability, visuomotor tracking, and psychomotor skills.
DEHYDRATION AND DELIRIUM
Dehydration is a risk factor for delirium and for delirium presenting as dementia in the elderly and in the very ill.
Recent work shows that dehydration is one of several predisposing factors for confusion observed in long-term-care residents.
GASTROINTESTINAL FUNCTION
Constipation, characterized by slow gastrointestinal transit, small, hard stools, and difficulty in passing stool, has a number of causes, including medication use, inadequate fiber intake, poor diet, and illness. Inadequate fluid consumption is touted as a common culprit in constipation, and increasing fluid intake is a frequently recommended treatment.
KIDNEY FUNCTION
In addition to regulating fluid balance, the kidneys require water for the filtration of waste from the bloodstream and excretion via urine. Water excretion via the kidney removes solutes from the blood.
The kidney is crucial in regulating water balance and blood pressure as well as removing waste from the body.
HEART FUNCTION AND HEMODYNAMIC RESPONSE
Blood volume, blood pressure, and heart rate are closely linked. Blood volume is normally tightly regulated by matching water intake and water output.
In healthy individuals, slight changes in heart rate and vasoconstriction act to balance the effect of normal fluctuations in blood volume on blood pressure. Decreases in blood volume can occur, through blood loss (or blood donation), or loss of body water through sweat, as seen with exercise. Blood volume is distributed differently relative to the position of the heart, whether supine or upright, and moving from one position to the other can lead to increased heart rate, a fall in blood pressure, and, in some cases, syncope.
Water intake acutely reduces heart rate and increases blood pressure in both normotensive and hypertensive individuals. These effects of water intake on the pressor effect and heart rate occur within 15–20 min of drinking water and can last for up to 60 min. Water ingestion is also beneficial in preventing vasovagal reaction with syncope in blood donors at high risk for post-donation syncope.
HEADACHE
Water deprivation and dehydration can lead to the development of headache. Although this observation is largely unexplored in the medical literature, some observational studies indicate that water deprivation, in addition to impairing concentration and increasing irritability, can serve as a trigger for migraine and can also prolong migraine. In those with water deprivation-induced headache, ingestion of water provided relief from headache in most individuals within 30 min to 3 h. It is proposed that water deprivation-induced headache is the result of intracranial dehydration and total plasma volume.
SKIN
The skin contains approximately 30% water, which contributes to plumpness, elasticity, and resiliency. The overlapping cellular structure of the stratum corneum and lipid content of the skin serves as “waterproofing†for the body. Loss of water through sweat is not indiscriminate across the total surface of the skin, but is carried out by eccrine sweat glands, which are evenly distributed over most of the body surface. Skin dryness is usually associated with exposure to dry air, prolonged contact with hot water and scrubbing with soap (both strip oils from the skin), medical conditions, and medications. While more serious levels of dehydration can be reflected in reduced skin turgor, with tenting of the skin acting as a flag for dehydration, overt skin turgor in individuals with adequate hydration is not altered. Water intake, particularly in individuals with low initial water intake, can improve skin thickness and density as measured by sonogram, offsets transepidermal water loss, and can improve skin hydration. Adequate skin hydration, however, is not sufficient to prevent wrinkles or other signs of aging, which are related to genetics and to sun and environmental damage. Of more utility to individuals already consuming adequate fluids is the use of topical emollients; these will improve skin barrier function and improve the look and feel of dry skin.
FATIGUE
A pair of recent studies found that young people who were mildly dehydrated were much more likely to feel fatigued during moderate exercise and even when sedentary. Unsurprisingly, fatigue is a common dehydration symptom, and it’s said to be the No. 1 cause of midday fatigue. [iv, v]
METABOLISM
Although the evidence is limited, your metabolism could benefit from drinking cold water. In fact, one study found that drinking cold water helped boost healthy men and women’s metabolic rate by 30 percent. The researchers concluded that the body expended more energy heating the cold water, which resulted in the boost in metabolism. [vi]
HYDRATION AND CHRONIC DISEASES
Many chronic diseases have multifactorial origins. In particular, differences in lifestyle and the impact of environment are known to be involved and constitute risk factors that are still being evaluated. Water is quantitatively the most important nutrient. In the past, scientific interest with regard to water metabolism was mainly directed toward the extremes of severe dehydration and water intoxication. There is evidence, however, that mild dehydration may also account for some morbidities. [iii]
Summary of evidence for association of hydration status with chronic diseases. [https://academic.oup.com/view-large/112300689]
Categories of evidence used in evaluating the quality of reports. [https://academic.oup.com/view-large/112300687]
WATER REQUIREMENTS
Several factors affect daily water intake. They include size of the body, activity level, diets, environmental temperature, and health conditions such as fever, diarrhea, and kidney diseases. Even though an average person loses 2.2 L of water daily, he requires only 2 L of water daily, as the body produces about 200 ml of water daily. It is called “metabolic waterâ€, which comes from the catabolism of macronutrients and chemical reactions taken place in the body.
SIMPLE EQUATION TO CALCULATE AVERAGE DAILY WATER INTAKE
AVERAGE DAILY WATER INTAKE =
250ml (Body Wt. in lbs. / 16)
+ 250ml (Total mg of Caffeine / 60mg)
+ Total lbs. Lost During Exercise (500ml)
The three sources of water are liquids, foods, and metabolic water. Milk and juices contain considerable water, but they do not count as the same volume of water. Not only do not alcoholic beverages and caffeine – containing drinks such as coffee, tea, and sodas count as water, but also they require an increase in water intake, because they act as diuretics. See the following link for water content range in selected foods.
In order to maintain peak athletic performance and achieve adequate recovery, it is mandatory to sustain the optimal level of hydration not only before exercise but also throughout the exercise. Dehydration causes a decline in peak athletic performance, hindering athletes to excel. In general, a simple guideline would be as follow:
Drink at least 2 liters throughout the day.
2 hours before exercise: 2 glasses of water.
1 hour before exercise: 1 glass of water.
30 minutes before exercise: 1 glass of water.
20 minutes before exercise: 1 glass of water.
10 minutes before exercise: 1 glass of water.
WATER INTAKE DURING EXERCISE
In order to keep the body fully hydrated during training sessions, you should drink ½ to 1 glass of water every 10 minutes. If you are not thirty, it does not mean that you are not dehydrated. Because thirst is not a good sign of how much hydrated you are.
Practically, athletes are taught to evaluate their hydration levels by using the two following guidelines:
Urgent feeling to urinate during or immediately after training. If you do not have the urge to urinate during your exercise session or within few minutes after exercise, it is a good and reliable sign that you have not taken enough water during your exercise session.
Color of the urine. This is not as reliable as the first sign. However, it is a useful indicator to assess hydration level. The urine is usually clear like water or slightly yellow. If the color of the urine is strong yellow or orange – colored, it could be a sign of not having enough water during exercise. You should bear in mind that taking some supplements or medications could affect the color of urine. For example, vitamin B2 (riboflavin) makes the color of urine strong yellow.
There are other factors that determine the degree of dehydration during exercise, and they include intensity of exercise, temperature and humidity of exercising environment, and strength or endurance training. Endurance athletes are more prone to dehydration than strength athletes. Regardless of what the sport is, an optimal hydration is a key to athletic excellence, and dehydration can significantly impair athletic performance and even increase tendency to sports injuries.
WATER INTAKE AFTER EXERCISE
The amount of water required during early post – workout period is at least 2 glasses (500 ml) or 2 glasses of water per one pound weight lost, whichever counts higher.
If your goal is getting leaner, dropping more body fat, or losing weight, you should always wait the whole 30 minutes, giving enough time for your body to continue burning fat unless you feel dizzy or lightheaded.
If your goal is not losing weight, and you want to build more muscles and increase your size, then you should not wait, and you may proceed immediately to the next period and follow the advices over there.
CONCLUSION
Water is the most essential component to every living organism. With 75% of American’s being chronically dehydrated it is important that we stress the importance of decreasing that statistic. Chronic dehydration can cause significant impairments/ deficits and dysfunction. It is especially important to hydrate before, during and after exercise; as well as in extreme environments.
I challenge my patients to follow the above water intake recommendations for at least 2 weeks to notice the difference! You may feel the need to urinate all the time at first but your body will adapt to being properly hydrated after time. Of course, if you have any existing condition or disease that may be affected by water intake, please consult your physician prior to starting this program. To simplify things, this is the equation to follow:
REFERENCE FORMULA
AVERAGE DAILY WATER INTAKE =
250ml (Body Wt. in lbs. / 16)
+ 250ml (Total mg of Caffeine / 60mg)
+ Total lbs. Lost During Exercise (500ml)
+ Water intake before exercise (2 hours before exercise: 500ml of water, 1 hour before exercise: 250ml of water, 30 minutes before exercise: 250ml of water, 20 minutes before exercise: 250ml of water, 10 minutes before exercise: 250ml of water.
+ Water intake during exercise (125 to 250ml of water every 10 minutes of exercise)
Let us know your thoughts and your experience!
________________________________
REFERENCES
[i] Survey of 3003 Americans, Nutrition Information Center, New York Hospital-Cornell Medical Center (April 14, 1998).[ii] Canadian Academy of Sports Nutrition (2014).[iii] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2908954/[iv] Ganio, M. S., Armstrong, L. E., Et. Al (2011). Mild dehydration impairs cognitive performance and mood of men. British journal of Nutrition, 106(10), 1535-1543.
[v] Armstrong, L. E., Et. Al (2012). Mild dehydration affects mood in healthy young women. The Journal of nutrition, 142(2), 382-388.[vi] Boschmann, M, Et. Al (2003). Water-induced thermogenesis. The Journal of Clinical Endocrinology & Metabolism, 88(12), 6015-6019.
Osteoarthritis is a common disease affecting millions of people around the world each year and is one of the leading causes of disability. The prevalence of OA progressively increases with age; however, only 25-30 per cent of people are symptomatic!
WHAT IS OSTEOARTHRITIS?
PATHOLOGICALLY, IT MAY BE DEFINED AS A CONDITION OF SYNOVIAL JOINTS CHARACTERISED BY FOCAL LOSS OF ARTICULAR HYALINE CARTILAGE WITH PROLIFERATION OF NEW BONE AND REMODELLING OF JOINT CONTOUR. IT IS A DYNAMIC REPAIR PROCESS THAT MAY BE TRIGGERED BY A VARIETY OF INSULTS, SOME MAY RESULT IN SYMPTOMATIC ‘JOINT FAILURE’ IN LAY MAN’S TERMS, OA IS JOINT DEGENERATION AND CARTILAGE LOSS. IT IS BY FAR THE MOST COMMON FORM OF ARTHRITIS.
RISK FACTORS
GENETIC FACTORS
OA KNEE PREVALENT IN ALL RACIAL GROUPS
HIP, HAND AND GENERALIZED OA ARE PARTICULARLY PREVALENT IN CAUCASIONS
MORE PREVALENT AND MORE COMMONLY SYMPTOMATIC IN WOMEN
EXCEPT AT THE HIP WHERE MEN ARE EQUALLY AFFECTED
TRAUMA AND OCCUPATIONAL HAZARDS
EXAMPLE FOOTBALL PLAYERS WITH KNEE OA, FARMERS WITH HIP OA, ETC.
AGING: LAXITY OF LIGAMENTS INCREASES WITH AGE
OBESITY
NEUROPATHY
DEPOSITION DISEASES: ANY SUBSTANCE THAT SITS INSIDE THE JOINT FOR TOO LONG FORMS DEPOSITS EXAMPLE: URIC ACID (GOUT)
ETOLOGY AND PATHOGENISIS
STAGES OF KNEE OA
CARTILAGE CHANGES: CHRONDROCYTES INCREASE PRODUCTION OF MATRIC COMPONENTS AND THE TURNOVER OF AGGRECAN COMPONENTS IS INCREASED BUT CONCENTRATION FALLS, LEADS TO INCREASED WATER AND SWELLING PRESSURE IN CARTILAGE, MAKING THE CARTILAGE VULNERABLE TO LOAD BEARING INJURY. FISSURING OF THE CARTILAGE SURFACE (‘FIBRILLATION’) EVENTUALLY OCCURS, LEADING TO THE DEVELOPMENT OF DEEP VERTICAL CLEFS.
BONE CHANGES: THE SUBCHRONDRAL BONE SHOWS A MIXTURE OF OSTEOLYSIS AND OSTEOSCLEROSIS, WHICH REFLECTS HEALED TRABECULAR MICROFRACTURES. SUBCHRONDRAL ‘CYSTS’ DEVELOP AS THE RESULT OF SMALL AREAS OF OSTEONECROSIS CAUSED BY THE INCREASED PRESSURE IN BONE AS THE CARTILAGE FAILS. OSTEOPHYTES: RESULT FROM PRODUCTION OF NEW FIBROCARTILAGE AT THE JOINT MARGIN WHICH UNDERGOES ENDOCHONDRAL OSSIFICATION.
CLINICAL FEATURES OF KNEE OA: TARGETS THE PATELLO-FEMORAL AND MEDIAL SIDE OF THE KNEE. ISOLATED OR AS PART OF GENERALISED OA. MOSTLY BILATERAL AND SYMMETRICAL. TRAUMA IS AN IMPORTANT RISK FACTOR IN MEN.
TREATMENT
ALTHOUGH THERE ARE NO TO LITTLE SCIENTIFIC EVIDENCE TO SUPPORT THAT ANY TREATMENT WILL RESTORE ANY DEGENERATION THAT HAS BEEN LOST DUE TO OA – THERE ARE TREATMENTS TO HELP WITH MANAGEMENT OF SYMPTOMS.
FULL EXPLANATION OF THE CONDITION.
INCLUDE RELEVANT RISK FACTORS (OBESITY, HEREDITY, TRAUMA); THE FACT THAT PAIN AND FUNCTION CAN IMPROVE DESPITE STRUCTURAL DAMAGE; DISCUSSION OF PROGNOSIS (GOOD FOR NODAL HAND OA, MORE OPTIMISTIC FOR KNEE THAN HIP OA); AND THE FACT THAT APPROPRIATE ACTION CAN IMPROVE THE PROGNOSIS OF LARGE JOINT OA.
EXERCISE.BOTH STRENGTHENING AND AEROBIC. -> AQUATIC EXERCISE IS THE BEST FORM!!!
I UNDERSTAND THAT THE COMMUNITY POOLS ARE CLOSED RIGHT NOW BUT IF YOU DO HAVE ACCESS TRY SWIMMING AND AQUATIC EXERCISE!
DRUG TREATMENT. (PARACETAMOL, NSAID OR OPIATES. INTRA-ARTICULAR CORTICOSTEROID INJECTION).
SURGERY. OSTEOTOMY OR JOINT REPLACEMENT.
NEUTRACEUTICALS
MANUAL THERAPY – CHIROPRACTIC, OSTEOPATHY, MASSAGE THERAPY, ETC.
PHYSIOTHERAPY MODALITIES
WEIGHT LOSS
JOINT SUPPORTS (ORTHOPEDIC BRACES)
ACUPUNCTURE
NEUTRACEUTICALS AND NUTRITION FOR ALL AREAS OF OSTEOARTHRITIS
PROPER NUTRITION AND SUPPLEMENTATION FOR OA SHOULD BE BASED AROUND THE FOLLOWING: REDUCE PAIN, DECREASE INFLAMMATION, IMPROVE FLEXIBILITY, HELP REPAIR CARTILAGE, ACCELERATE HEALING PROCESS.
1. DECREASED SYNOVIAL FLUID
SYMPTOMS
PAIN
JOINT STIFFNESS
LOSS OF FLEXIBILITY
CRACKING OR POPPING SOUND*
DIETARY RECOMMENDATIONS
DRINK MORE THAN 3 LITERS A DAY!!! •REMEMBER, FOOD HAS WATER IN IT TOO!
GENERALIZED DAILY WATER INTAKE FORMULA
= 250ML X (BODY WEIGHT IN LBS. / 16) + 250ML (TOTAL MG OF CAFFEINE / 60MG) + TOTAL LBS. LOST DURING EXERCISE X 500ML
HYALURONIC ACID
TAKE 100 – 200MG PER DAY. •HELPS TO INCREASE THE PRODUCTION OF SYNOVIAL FLUID, IMPROVING JOINT FLEXIBILITY.
2. DECREASED CARTILAGE
NEUTRACEUTICAL RECOMMENDATIONS
GLUCOSAMINE
SOURCES: MADE SYNTHETICALLY OR FROM SHELLS OF SHRIMP, CRAB, LOBSTER
REDUCES PAIN AND INFLAMMATION
HELPS TO REPAIR CARTILAGE AND INHIBITS JOINT DEGENERATION
DOSAGE: 1500 – 2000 MG/DAY FOR AT LEAST 6 WEEKS AT A TIME
SIDE EFFECTS: STOMACH DISTRESS, DIARRHEA, INSULIN RESISTANCE (BLOOD SUGAR RISES), NaCL (BLOOD PRESSURE AFFECTED), CAN THIN BLOOD
LESS EFFECTIVE IF TAKEN WITH TYLONEL
ACETAMINOPHEN (TYLONEL) METABOLIZES USING SULFATE, THUS REDUCING THE PAIN RELIEVING EFFECTS OF GLUCOSAMINE SYNTHESIS
REQUIRES A SULFUR BASE FOR REBUILDING AND REPAIRING CARTILAGE
WHEN COMBINED WITH CHRONDOITIN SULFATE, IT IS JUST AS EFFECTIVE AS CELEBREX MEDICATION.
CHRONROITIN SULFATE
NATURALLY FOUND IN CARTILAGE AND TENDONS
DECREASES PAIN AND DECREASES INFLAMMATION
INHIBITS JOINT DEGRADATION (BREAKDOWN).
SOURCES: COW’S CARTILAGE AND SHARK’S CARTILAGE SIDE EFFECTS: HIGH DOSES RESULT IN NAUSEA AND DIARRHEA (<10G)
DOSAGE: 1200 MG/DAY
MSM (METHYLSULFONYLMETHANE)
NATURALLY FOUND IN THE BODY AND MANY FOODS, ESPECIALLY GREEN VEGETABLES
REDUCES INFLAMMATION AND PAIN
USE IN COMBINATION WITH GLUCOSAMINE.
GOOD SOURCE OF SULFUR
DOSAGE: 250 – 500MG /DAY
MAY TAKE UP TO 6000MG/ DAY
SIDE EFFECTS: MILD BLOOD-THINNING EFFECT
CAPSAICIN
ACTIVE COMPONENT OF CHILI PEPPER
BLOCKS THE RELEASE OF SUBSTANCE – P
A NEUROPEPTIDE ACTING AS A NEUROTRANSMITTER AND NEUROMODULATOR FOR TERMINALS OF THE SENSORY NERVES ASSOCIATED WITH PAIN AND INFLAMMATION.
DOSAGE: APPLY TOPICAL CREAM SPARINGLY 3-4 TIMES PER DAY AS NEEDED.
NOT ROUTINELY USED IN THE TREATMENT OF OA
L – PROLINE AND L – LYSINE
BOTH AMINO ACIDS
IMPROVE COLLAGEN PRODUCTION
L-LYSINE
INCREASES GH
HELPS REPAIR CARTILAGE IN OA
ALSO PREVENTS FROM COLD SORES
ESSENTIAL AMINO ACID
DOSAGE: 1000 – 1500 MG/ DAY
L-PROLINE
NON ESSENTIAL AMINO ACID
ALSO HELPS WITH TISSUE AND WOUND HEALING
DOSAGE: 500 – 1000 MG / DAY
VITAMIN C
IMPORTANT IN THE CONVERSION OF PROLINE AND LYSINE TO HYDROXYPROLINE AND HYDROXYLYSINE, WHICH ARE THE KEY CONSTITUENTS OF COLLAGEN
DOSAGE: 2 – 3 GRAMS /DAY
BOSWELLIA EXTRACT
IMPROVES BLOOD SUPPLY TO THE JOINT TISSUES AND REDUCES INFLAMMATION
HELPS PREVENT CARTILAGE LOSS
ANALGESIC PROPERTIES
DOSAGE: 1200MG / DAY
STUDIES SHOW SIGNIFICANTLY REDUCES OA PAIN AND FUNCTION WITHIN 7 DAYS AND SLOWED CARTILAGE DAMAGE AFTER 3 MONTHS.
CURCUMIN
IMPORTANT IN THE CONVERSION OF PROLINE AND LYSINE TO HYDROXYPROLINE AND HYDROXYLYSINE, WHICH ARE THE KEY CONSTITUENTS OF COLLAGEN
DOSAGE: 2 – 3 GRAMS /DAY
IT IS IMPORTANT TO NOTE THAT BEFORE STARTING ANY DIET OR SUPPLEMENTS, THAT YOU MAKE SURE THAT IT IS SAFE FOR YOU TO DO SO BY TALKING WITH YOUR HEALTHCARE PROVIDER.
IF YOU WOULD LIKE TO DISCUSS AND START TAKING NEUTRACEUTICALS FOR OSTEOARTHRITIS OR ANY OTHER CONDITION, LET US KNOW AND WE WILL BE ABLE TO ASSIST YOU.
WE HAVE PARTNERED WITH “FULL SCRIPT” AND ARE ABLE TO PRESCRIBE CUSTOMIZED NEUTRACEUTICALS WHICH YOU CAN PURHCASE DIRECTLY FROM YOUR PERSONAL PORTAL ONCE WE’VE SENT YOU AN EMAIL PRESCRIPTION. THEY WILL DELIVER THEM TO YOUR HOUSE SO YOU CAN STILL KEEP IN CHECK WITH QUARENTINE REGULATIONS!
IF YOU HAVE ANY QUESTIONS, COMMENTS OR CONCERNS,PLEASE REACH OUT TO US!
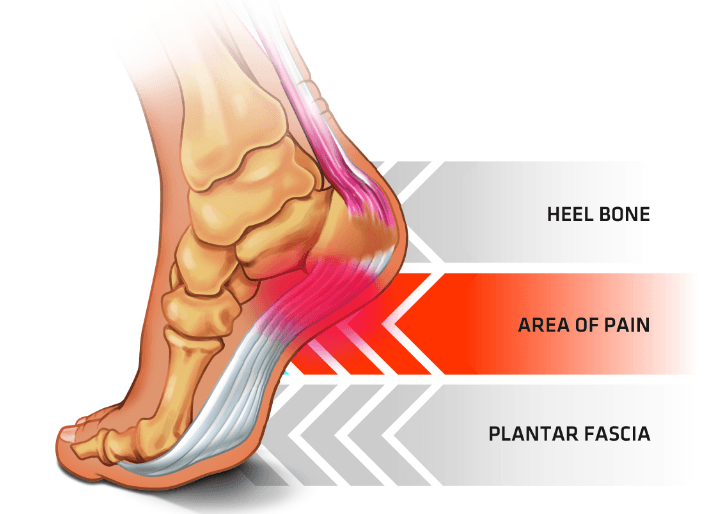
* Pain can radiate throughout the plantar fascia towards the toes.
Plantar Fasciitis goes hand in hand with the idea that during this quarentine, people are going to be looking for ways to be active without going to the gym – running, walking, home HIIT workouts, etc.
Plantar fasciitis occurs when tension within the plantar fascia increases.
The plantar fascia is designed to absorb the high stresses and strains we place on our feet. But, sometimes, too much pressure damages or tears the tissues. The body’s natural response to injury is inflammation, which results in the heel pain and stiffness of plantar fasciitis.
Common cause of foot pain in adults, peak incidence between the ages of 40 and 60 years. Also in younger population consisting of runners, aerobic exercise dancers, and ballet dancers. Resolution of symptoms occurs within 12 months in more than 80% of patients. The exact incidence and prevalence of plantar fasciitis by age are unknown, but estimates do show that approximately one million patient visits per year are due to plantar fasciitis. This condition accounts for about 10% of runner-related injuries and 11% to 15% of all foot symptoms requiring professional medical care. It is thought to occur in about 10% of the general population as well, with 83% of these patients being active working adults between the ages of 25 and 65 years old.
SYMPTOMS
Severe pain with the first steps on arising in the morning, usually lessens with weight-bearing activity during the day. Worse on walking barefoot or up stairs.
Characteristic: Dull tooth-ache or burning pain, Stiffness may also be present, Pain Location: Posterior and medial aspect of heel, Medial tubercle of calcaneus, Medial longitudinal arch, Both heels often affected, Pain worse with first few steps in morning, Pain may be worse at days end in severe cases, Pain worse with first steps of run, Pain worse with prolonged standing (weight bearing).
TREATMENT
Common treatments healthcare professionals may prescribe for Plantar Fasciitis include chiropractic treatment, osteopathy, physiotherapy, iontophoresis, radial shockwave therapy, physical therapy, electrotherapy, ultrasound therapy, NSAIDs, orthotic foot support, surgery (rare cases) and more.
HOME TREATMENT
These are a few tips in managing Plantar Fasciitis at home during this quarantine… until we can see you for clinical treatment.
REST – now in a perfect world I would have you completely stop doing the activity which is causing your pain until the acute phase subsides a bit; however, these are not perfect times and I believe that stopping physical activity completely would be worse for you in the long run. So, I’m willing to compromise by advising you to decrease to amount which you are exercising (decrease miles and intensity on a run/walk), substitute exercises which pound/stress the foot (like jumping during HIIT training) with exercises which reduce the pounding/stress, and of course do all the below recommendations!
DIRECT ICE – Freeze a styrofoam or dixie cup with water. Peel away an end so ice is showing and you have a “handle” on one end. Directly massage the ice on the most painful area in small, continuous circles so the ice melts on your skin. IT WILL BE COLD AND SOMETIMES PAINFUL. Do this for no longer than 2 minutes as doing it for longer will put your skin at risk for complications.
This tricks the cells into thinking they need to constrict and protect themselves for “survival”. Almost like how cells react when someone falls into a frozen lake. As soon as the ice is over, the cells realize they need to “save” the area by increasing oxygen and blood supply to the area which will help speed up recovery of the injured area.
TENS – before, after exercising and PRN throughout the day. I find a combination of Heat over TENS before exercise and Ice with TENS after exercise really helps with pain management. See below for common TENS placement.
WEAR YOUR ORTHOTICS – even if it’s inside the house
NIGHT SPLINT – see below image for a version of a homemade night splint using athletic tape if you do not have access to a proper night splint.
TAPING – see below image for athletic tape method or visit this link for kinesiology taping method. I find during the acute phase (most painful and inflamed) that the athletic taping does a better job in support but when it subsides a bit and you start exercising more the kinesiology tape will help better without restricting motion.
Again, if you have any questions, comments or concerns, please do not hesitate to contact us. We will be happy to help in any way we can during this novel time.
It pains us to say this but unfortunately due to the updates surrounding COVID-19, we are following the recommendations set forth by our colleges, associations, Health Canada and government to practice social distancing and close the clinic for another week. Again, we are playing this week by week – hopefully, if we all do our part we can start accepting appointments soon.
As you know, we have been coming up with pain management articles for common conditions and posting those daily. Everyday during this quarantine, expect a new article to be released which will be sent directly to your email and posted on our social media pages. Please follow our pages for our latest updates.
Facebook and Instagram: @cccosteopathy & @communitychiropracticcenter
Do you have any topics or injury management tips you’d like us to comment on? If so, let us know by emailing us, sending us a DM or commenting on social media pages.
HINT: MONDAY’S ARTICLE IS ON PLANTAR FASCIITIS AND WILL BE RELEASED AT 9AM EST.
Does this picture look like you? Maybe you are forced to work from home without the proper ergonomics or simply been trying to fill out your EI for hours and hours… Either way, we got you!
Having tension in your neck/ shoulder areas is a struggle that many people encounter on a daily basis – with and without quarantine. This is primarily due to posture while sitting at a computer desk for long periods of time.
While there are many underlying pathologies like decreased cervical lordosis, arthritis, etc. that play a role in this pain cycle, there are some tips that you can do right now to help manage your pain.
HOME TREATMENT
HEAT – use a moist heat pad on your neck and shoulders throughout the day. Even when you are at the computer.
FIX YOUR ERGONOMICS – In going along with the philosophy of treating the cause, not just the symptoms, if you don’t correct the variable that is causing you pain, no matter what you do, the pain will eventually return.
TENS – use your TENS machine PRN (as needed). I like to use the TENS with heat over top of it for maximum relief for this condition.
THORACIC STABILIZER – If we have already dispensed a thoracic stabilizer to you, get back to using it. Start doing to program which came in the box when you got it. If you can’t find it, here is the link for the manual.
CERVICAL ORTHOSIS – If you have been diagnosed with decreased cervical lordosis and been prescribed and dispensed a cervical orthosis, use it the way you were prescribed.
It is important to note that, the above treatment options, although can help manage pain for most patients, the underlying cause must be corrected or else the pain cycle will continue. Hopefully, we are back soon so we assess your situation, identify your specific issues and develop a customized treatment program.
If you have any questions, comments or concerns, please do not hesitate to contact us!
With the gym’s closed, many of you might find yourself trying to exercise at home and outside and many of you have began or thought of running or walking outside now that the weather is finally cooperating. AND FINALLY, many of you might feel pain in your knee(s) during and after running.
In fact, 25% of the general population suffers, or has suffered, from a little known cause of knee pain called patellofemoral pain syndrome. It is the most common overuse knee injury among runners, and it can account for up to 40% of the knee complaints in sports medicine clinics. This makes Patellofemoral Pain Syndrome the most common knee pathology when it comes to knee injuries in runners.
Patellofemoral Pain Syndrome is often called Runner’s knee and sometimes called Chondromalcia. Chondromalcia means “softening of the cartilage under the knee cap; however, This term is not used much anymore as there is no real softening.
It is one of the most common causes of knee pain in all age groups, including teens and young adults.
Common in runners, yet is seen in soccer players, gymnasts, cyclists, rowers, tennis players, ballet dancers, basketball players, and volleyball players.
CAUSES OF RUNNER’S KNEE
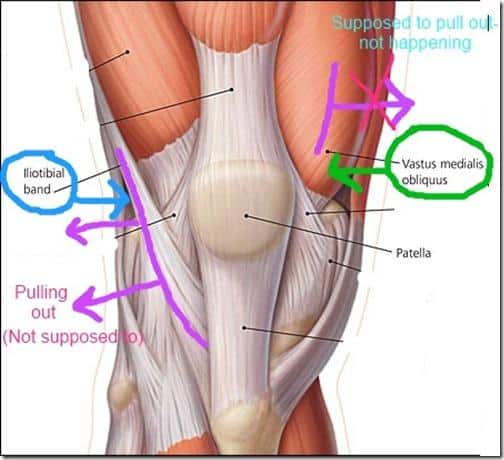
Runner`s knee is due to an irritation and side-to-side movements of the kneecap (patella) on the groove in the femur. Possible causes include:
Poor kneecap tracking (maltracking) – the common cause
Weak Quadriceps.
Imbalanced Quadriceps.
Weak Hamstrings
Tight Iliotibial Band.
Weak Hip Abductors
Tight iliotibial band.
Neuromas.
Bursitis.
Overuse.
SYMPTOMS:
Pain: in front, around or beneath the kneecap. The pain is usually perceived maximally when the knee comes to within 15-20 degrees of full extension.
More pain and/or feeling of joint instability after climbing stairs, jumping rope, running, or after a prolonged sitting, like for a movie, and so it is also called “movie sign” or “theater sign.
Sometimes a clicking, cracking or crunching sound is heard when the knee is bent or straightened. This is the kneecap slipping back into the groove.
TREATMENT:
RICE.
Activity modification: avoid activities that cause extra stress on the knees such as squatting/kneeling or high impact activities like running until the pain subsides. Swimming is safe.
Anti-inflammatory medications: PRN (Pro Re Nata); a Latin phrase meaning “if neededâ€.
Therapeutic exercises/ physiotherapy.
Electrotherapy
Low Level Laser Therapy
Ultrasound Therapy
Radial Shockwave Therapy
Cryotherapy
Osteopathy
Taping of the knee.
Proper Foot Wear: e.g. Shoes with an arch support to control over pronation, shoes with adequate cushioning in sole to help absorb shock. Orthotics may be required for those with severe over pronation. Limit the time spent wearing high heels.
Knee brace.
Surgery.
QUARANTINE TREATMENT
With limited treatment options available, these are a few home treatment options which you can implement.
RICE (REST, ICE, COMPRESSION, ELEVATION)
However, only ice PRN (if needed) directly after running or exercising. Do not ice before exercise.
TENS – before, after exercising and PRN throughout the day. I find a combination of Heat over TENS before exercise and Ice with TENS after exercise really helps with pain management.
Natural Vasodilation/ Vasoconstriction:
Heat and ice both work using the same mechanism by changing the amount of blood flow to the affected area, but with opposite results. Â When ice is applied to tissue, the blood vessels in that area will get smaller. Â This is called vasoconstriction and decreases the amount of blood that can reach the tissue. Â When heat is applied, the blood vessels in that area will get wider. Â This is called vasodilation and will increase the amount of blood that can reach the tissue.
I find this a great method to reduce acute and chronic inflammation, reduce pain, and increase the speed of recovery.
METHOD: Do the following in sequential order, ending with only 2 minutes ice.
10 min ice, followed by 10 min heat
8 min ice, followed by 8 min heat
6 min ice, followed by 6 min heat
4 min ice, followed by 4 min heat
2 min ice, followed by 2 min heat
2 min ice
Direct ice – Freeze a styrofoam or dixie cup with water. Peel away an end so ice is showing and you have a “handle” on one end. Directly massage the ice on the most painful area in small, continuous circles so the ice melts on your skin. IT WILL BE COLD AND SOMETIMES PAINFUL. Do this for no longer than 2 minutes as doing it for longer will put your skin at risk for complications.
This tricks the cells into thinking they need to constrict and protect themselves for “survival”. Almost like how cells react when someone falls into a frozen lake. As soon as the ice is over, the cells realize they need to “save” the area by increasing oxygen and blood supply to the area which will help speed up recovery of the injured area.
Even if you do not suffer from Patellofemoral pain syndrome, try some of these exercises out to help prevent it. For prevention, I like to look at glute strength, hip stability, and knee stability. A good exercise for knee control is the Terminal Knee Extension.
If you have any questions, comments or concerns, please let us know and we will try and help as much as we can during this time.
Again, for the most up-to-date information follow us on Facebook and Instagram. @CCCOsteopathy and @CommunityChiropracticCenter
We know that these are tough times, psychologically, emotionally, financially and physically. They all play a role our overall health. There is a strong connection between physical health and psychological health – by exercising daily, doing mobility exercises and eating healthy we can reduce our physical and psychological stress which will put us in a better place for when we can get our lives back on track.
Again, if any of the exercises hurt too much, please stop and reach out to us. If you are unsure if you should be doing these exercises, before you start them, please reach out to us so we can guide you.
The guy is a wizard. I’ve been looking for a long time for someone that knows what they’re doing when it comes to backs. I will only see Spencer now going forward. If you decide to see someone else for back pain I’m not sure if you really want to get better. Whole clinic is great.
After many years of cervical spine discomfort and osteoarthritis most likely as a result of sitting at a desk for a good number of years, I found myself wanting to find an alternative means towards improving my spine health!My Naturopath Doctor recommended I see an Oesteopath namely Spencer Jean who came highly recommended.Spencer welcomed me into his office and the conversation began as to how to go about the process of correcting my posture! A plan of attack was formulated as to how to begin the process which was amazingly positive based on his confidence in doing so along with my part in wanting to do so!Today my posture has improved tremendously and I cannot thank Spencer enough for getting me to this point! The exercises are not difficult and As I see the progress, I am so much more encouraged in doing so! Thank you so much Spencer and the wonderful welcoming staff at Community Chiropractic Centre! I am truly blessed!
Spencer has been a great benefit to me, as he listens to what is wrong and works to help with that problem; so that I get some relief & can do more of my ADL. Before meeting Spencer & being under his care; I had very limited relief of discomfort. I would recommend anyone with chronic pain & skeletal ailments to give Spencer a try. He maybe just what you need in your life.
Spencer is great! Very professional and caring. After years of chronic back pain, I can honestly say I feel better after every visit. The office staff is friendly and very easy to deal with!
Spencer is an amazing osteopath. I brought my 3 week old to see him for colic and he has helped her immensely! She is now 3 months and doing so well. Spencer is fantastic with babies. He is so caring and my little just adores him! Highly recommend his service.
I actually love going to see Spencer. He addresses my problems and I'm not sitting around for hours past my appointment time waiting to see him. In and out within 30 minutes. He takes care of my kids as well. I would recommend him to anyone without hesitation.Thanks for keeping us all in one piece and keeping us at our 100% for our tournaments.
‹
›
Copyright by Spencer Jean & Associates. All rights reserved.